On Wednesday, February 19th, 2020, at 9:54PM, the following email was received in Mon4t’s contact mailbox:
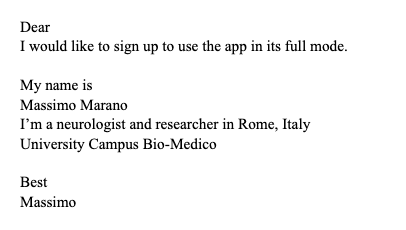
The following morning, I was already on Zoom with Dr. Marano learning that he was looking for a solution to examine patients for research he was conducting. We set the test protocol he needed, and he could immediately start working – a big advantage for having a smartphone used as a medical device. Turns out, that the following day, February 21st, 2020, was “Day 1” in Italy, “patient one” is officially confirmed as a case of COVID-19 by Ospedale Sacco in Milano, mass testing of the population in the Codogno area starts. By the end of the day another 16 cases in Lombardy are confirmed, COVID-19 hits Italy, and the rest is history.
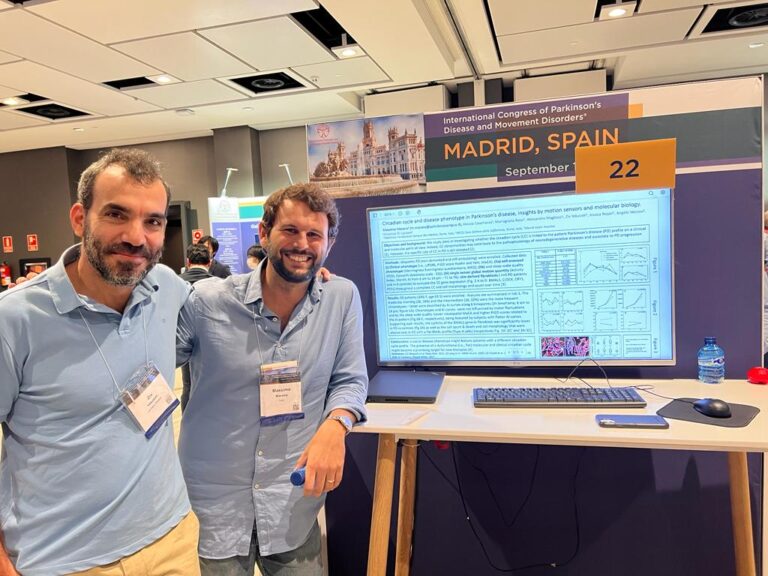
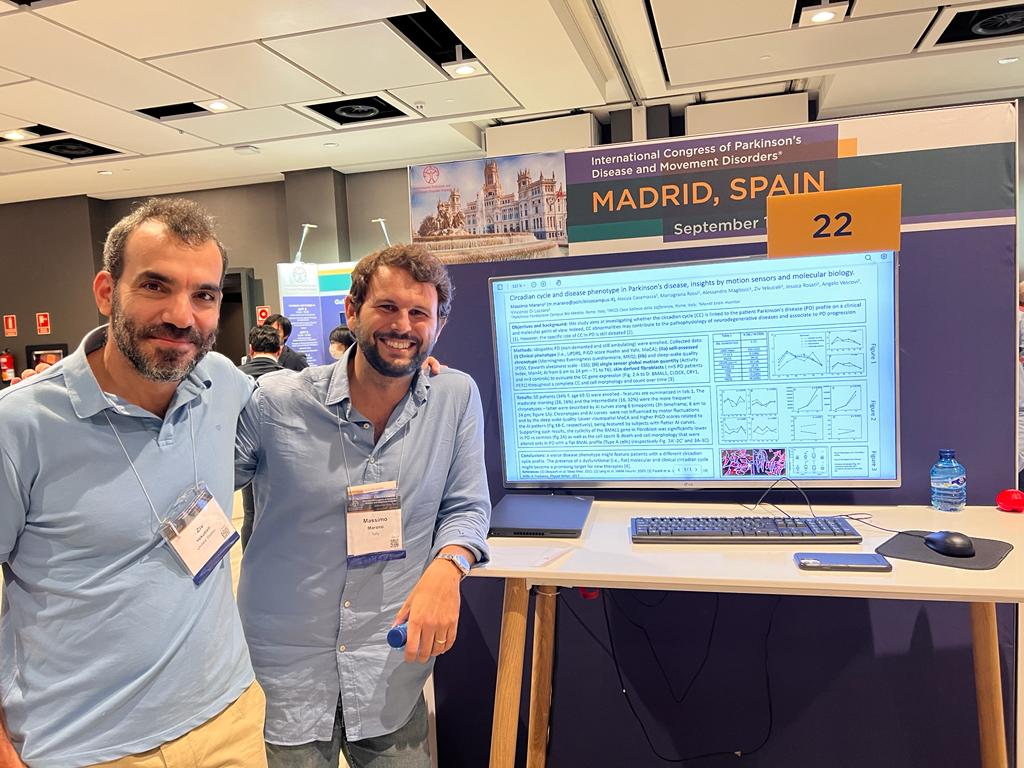
Israelis are known for our capability to quickly adapt and respond to rapid changes, improvising and fixing things on-the-fly. I can tell you that Dr. Marano and his team in Rome, showed us that they are just as capable. Within days, under lockdown that prevented them from seeing their patients, they quickly got Mon4t’s app up and running at the patient’s home. The results of this first-of-its-kind solution were published and since then expanded, leading to more collaborations. Finally, Dr. Marano and I met at the International Congress of Parkinson’s Disease and Movement Disorders (MDS), where he presented his latest results using Mon4t app, and more importantly, we had some time to share a couple of beers 🙂

Despite the challenge of coping with COVID, both teams in Israel and Italy were able to quickly adapt the technology and infrastructure to enable tele-neurology. Or maybe, it’s not despite of COVID, but because of it. COVID gave the tele-health business a huge boost, because it was almost impossible to practice medicine in any other way. With COVID on the decline, so are the numbers related to tele-health. Tele-health’s relevance and practice is still way above where we started before COVID, but it seems like the momentum has stopped.
At least in neurology I believe the reason for that is that tele-visits were considered as tele-neurology, which is not the case. Indeed, tele-visits save time to the patients, as they can be examined without the hassle of going to the clinic. On the other hand, tele-visits are making it more challenging for the neurologist to evaluate many of the symptoms, and some, gait for example, cannot be properly assessed over Zoom at all. Tele-visits still require the physician and patient to be present on the same call at the same time, and the visit lasts about the same time as the clinical visit. It’s no wonder then, that tele-visits have not decreased the neurologist’s backlog, if anything, they may have contributed to increasing it.
I believe that using technology to offer proper tele-neurology cannot rely solely on tele-visits. Rather, technology should be used to allow the neurological assessment to be conducted offline in an inclusive and quantitative manner, while capturing the patients’ symptoms in their daily lives. This will allow the physician to understand if an appointment is needed in the first place. If the treatment is working and the patient is stable, why schedule an appointment? If there is a reason for concern, why should a patient wait for an appointment to take place months later, which will worsen his condition and increase the risk of falls and other incidents. When there is an appointment, the neurologist should already have the test results needed, just like the report from a blood test or an ECG is ready for the cardiologist. This is what technology should offer.
Having demonstrated that our product is working in various settings, for different neurological conditions, we now focus on enabling tele-neurology as a service. With our existing leading-hospitals partners, Mon4t service will support preliminary screening of the patients, connecting them with the most suitable neurologist, monitoring their condition continuously, setting up an appointment when (and only when) needed, and support the treatment adjustment according to the quantitative results we provide. It’s up to us to show that doing so will not only reduce clinical and online visits, but also physician time per visit, hospital backlogs and emergency room visits, all while maintaining top quality-of-care for patients – I believe we can even improve it. Dr. Marano’s hospital will be one of several hospitals in which this transition will start taking place, if you are a neurologist or a medical administrator who wants to be a part of it too, please contact us!
Ziv Yekutieli PhD, Mon4t CEO